Over the last few weeks, we reviewed around 7-8 studies that clearly demonstrate that unvaccinated kids are healthier and more robust than vaccinated kids.
In other words, these studies are vax-unvax studies like we have been wanting for years!
These studies met these criteria:
1) includes a never-vaccinated control group. This control group has never received any vaccines.
2) includes a fully-vaccinated exposed group. This group must receive all or nearly all the vaccines in the CDC schedule.
3) measures long-term health outcomes, especially neurological and immune-related outcomes, such as autism, mental illnesses, learning disabilities, allergies, autoimmune disorders and the like. The follow-up period was and should be at least a couple of years, because it takes this long for these health conditions to appear.
This is even more substantiated by thousands of testimonials of moms who raise unvaccinated children.
And this is confirmed by several MDs and pediatricians who have
found the truth 😊
Now it is time to debunked studies that are the vaccine
promoters use to claim that vaccinated kids are healthier. Yes, you read it
right, they claim that vaccinated kids are healthier!
But I have got to meet a child who is fully vaccinated and never been on any kind of medication or prescription.
Vaccine promoters use 2 arguments to justify the refusal to study the never-vaccinated:
1) randomization is unethical because vaccines would need to be withheld from some subjects. Vaccines are so wonderful that it would be unethical to withhold them, even temporarily. This argument cracks me up because I know hundreds of parents who would be willing to be part of such a study because we know that vaccines hurt and destroy lives.
2) observational studies are useless because of selection bias. The
unvaccinated differ in many ways from those that choose to be vaccinated,
rendering the results meaningless.
The argument #2 is particularly hypocritical because almost all studies of vaccine safety are observational and therefore vulnerable to selection bias (and other biases).
Observational studies are done all the time, despite the selection bias problem. Concern about selection bias, while valid, is not a reason to not do research.
It is obvious that the vaccine promoters do not want a study to be done regarding the health status of vax vs unvax, because as we have seen, they would realized that vaccinated are sicker than unvaccinated.
They do not want their bubble to be burst 😊
Vaccine promoters believe that those 5 studies demonstrate without any doubts than vaccinated kids are healthier. But are they?
We shall see! 😊
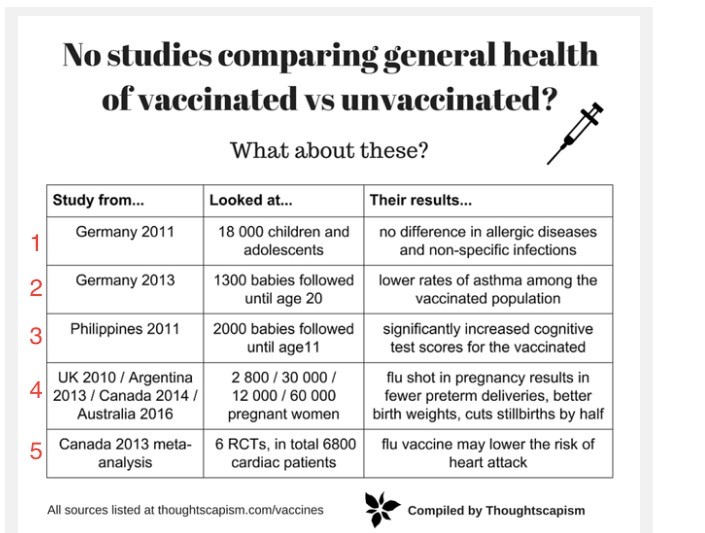
This is a list of alleged “vax-unvax” studies cited by vaccine promoters.
Studies 4-5 are not vax-unvax studies (as defined above based on the criteria
we defined) because they only looked at the flu vaccine. Studies 1-3 are
considered here.
Studies 4 and 5 are clearly not relevant because they are limited to the flu vaccine. The flu vaccine study results are almost certainly explained by healthy user bias.
Studies 1-3 are relevant because they consider multiple vaccines.
So, in the next few blogs we will look at studies 1-3 in detail.
1) Germany 2011. (Schmitz et al) Full paper: Vaccination Status and Health in Children and Adolescents
It is widely cited by vaccine promoters.
Adverse outcomes measured: Allergic rhinitis (respiratory allergy), eczema, asthma, and vaccine-preventable diseases (pertussis, measles, mumps, rubella).
Interestingly, there is no neurological or autoimmune outcomes considered, which would have been to include actually because there is an increasing number of evidence to indicate a direct correlation between vaccination and those conditions.
The study is not a vax-unvax study, as defined above. It has several problems that render it useless for measuring the health impact of the full vaccine schedule:
1) Neurological and autoimmune disorders were not measured.
2) Allergic disorders can take years to appear, and some vaccines are given
after age 1, so the 1-5 age group should be excluded. The study therefore
effectively had only n=50 (age 6-17) zero-vax subjects.
3) The vaccinated group is defined as receiving at least
one vaccine. This dilutes the vaccinated group with lightly-vaccinated
subjects.
4) The vaccinated group received an unknown number of vaccines. No details are
provided about vaccine exposure (e.g. an average number of vaccines received by
vaccinated subjects, or percentage that are fully vaccinated).
The vaccinated group may have had low vaccine utilization. Specifically, from Fig. 1, the percentages of “sufficiently vaccinated” subjects for each disease are:
Pertussis: 10,164/13,359 = 76%
Measles: 10,120/13,359 = 76%
Mumps: 9,789/13,359 = 73%
Rubella: 9,209/13,359 = 69%
These percentages are low compared to vaccination rates in the USA, for example.
The low vaccine use in the vaccinated group reduces the sensitivity of the study.
The low vaccine use may be due to the inclusion of young (e.g. ages 1-3) subjects, since subjects at this age are not fully vaccinated for these diseases.
Different subject-inclusion criteria were used for the 2 outcome categories:
1) vaccine-preventable illnesses, and
2) allergic disorders.
Specifically, for vaccine-preventable diseases, only sufficiently-vaccinated subjects were included.
For allergic disorders, all subjects were included, even those that were not sufficiently vaccinated.
This is a double-standard.
These different inclusion criteria reduce the detection of allergic disorders caused by vaccines and maximize the detection of vaccine efficacy.
The double-standard suggests the researchers had an agenda to bury evidence of harm and make vaccines look good.
Yep, it is basically epidemiology. Using statistics, it is easy to “hide” association and correlation. We see this being used regularly in studies looking at the association between autism and vaccination for example. If you do not want to see a correlation, you just change the criteria!
The paper states:
“Of the 17,641 individuals in this study, 14,148 children and adolescents were aged 1–17 years and lived in non-immigrant families.
A vaccination card was available for 13 499 of these individuals (95.4%).
Of these, 41 were not evaluated because their vaccination card was illegible or seemingly incomplete (follow-up document).
Furthermore, five unvaccinated subjects were not evaluated who, according to their parents, had not been vaccinated at the planned date because of frequent illnesses. Evaluable vaccination data were therefore available for 13 453 children and adolescents aged 1–17 years (95.1%).
For 94 of these children and adolescents, 48 girls and 46 boys, no vaccination had been documented at the time of this survey.”
So, the study compared 13,359 to 94 subjects (13,453 subjects total).
The large imbalance in group size means the statistical power is much lower than a comparison of equal group sizes (e.g. 9000 vs 9000 subjects).
So, describing the study as having 18,000 subjects is misleading to most people. It implies high statistical power, which is not the case.
The unvaccinated group was defined as having no documented vaccination.
That is not necessarily the same thing as documented affirmation of zero vaccine exposure.
Medical records are sometimes lost or misplaced, so children lacking documented vaccination may actually be vaccinated.
Only 0.6% of the study subjects were in the unvaccinated group.
Accordingly, even rare occurrences of lost records could put significant numbers of vaccinated subjects into the unvaccinated group.
Parents were not asked about vaccine exposure.
The paper says that parents were interviewed about their children’s health and possible confounders (e.g. education, income), but not vaccine exposure.
It seems strange that parents were not asked about the vaccination status of their children. Indeed, when the goal of this paper was to study the effect of vaccination on children’s health.
In view of these flaws, this study is essentially meaningless with regard to
the safety of the CDC vaccine schedule.
The biggest problems are the inadequate number of unvaccinated controls of age 6+ (50), the “at least one vaccine” definition for the vaccinated group, and no investigation of neurological or immune conditions.
This study therefore cannot be used as evidence of safety for the CDC vaccine schedule.
God bless y’all 🙂
Dr. Serge